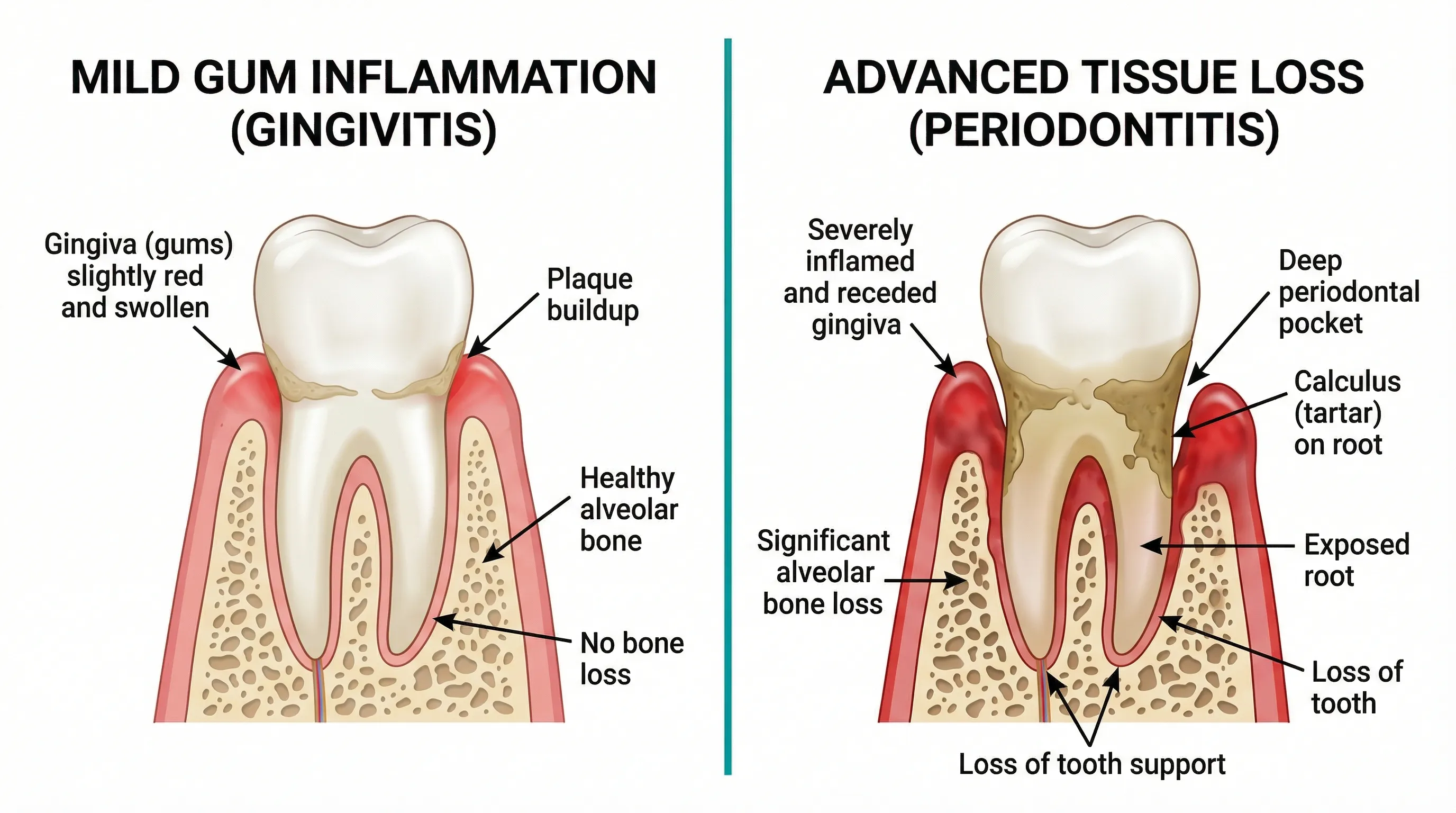
Gingivitis is the early, reversible stage of gum disease — red, swollen, bleeding gums with no bone loss. Periodontitis is the advanced, irreversible stage — deep pockets, bone destruction, and potential tooth loss. The critical difference: gingivitis can be completely reversed with proper care, while periodontitis damage is permanent and requires professional treatment. Catching gum disease at the gingivitis stage is the single most impactful thing you can do for your long-term oral health.
Gingivitis and periodontitis are not two separate diseases — they're two stages of the same disease continuum. Think of gingivitis as the warning light on your dashboard. Periodontitis is what happens when you ignore that warning for too long.
Understanding the differences between these conditions is essential for knowing when you can manage things at home and when you need professional intervention.
The Key Differences at a Glance
| Feature | Gingivitis | Periodontitis | |---------|-----------|---------------| | Severity | Mild (early stage) | Moderate to severe (advanced) | | Bone loss | No | Yes | | Pocket depth | 1-3mm (normal to slightly elevated) | 4mm+ (pathological) | | Reversible? | Yes — fully reversible | No — damage is permanent | | Tooth mobility | None | Possible in advanced stages | | Treatment | Improved hygiene + professional cleaning | Scaling/root planing, possibly surgery | | Pain | Usually painless | May be painless until advanced | | Prevalence | 50-90% of adults | 42% of adults 30+ (CDC) |
What Is Gingivitis?
Gingivitis is inflammation of the gingiva (gum tissue) caused by bacterial plaque accumulation along the gumline. It's the body's inflammatory response to the toxins produced by plaque bacteria.
Symptoms of Gingivitis
- Red gums — Healthy gums are coral pink; gingivitis gums appear red or dark pink
- Swelling — Gum tissue becomes puffy, particularly between teeth (interdental papillae)
- Bleeding — Gums bleed during brushing or flossing, or when probed by a dentist
- Bad breath — Bacterial toxins produce volatile sulfur compounds
- No pain — Gingivitis is typically painless, which is why many people don't realize they have it
What's Happening at the Tissue Level
When plaque accumulates along the gumline, bacteria (particularly Fusobacterium nucleatum and Prevotella intermedia) produce endotoxins that penetrate the gum tissue. Your immune system responds with inflammation:
- Blood vessels dilate, increasing blood flow (causing redness)
- Capillary walls become more permeable (causing swelling)
- Immune cells flood the area to fight bacteria
- The inflamed, engorged tissue bleeds easily when disturbed
Critically, the junctional epithelium — the seal between your gum and tooth — remains intact. The periodontal ligament and alveolar bone are unaffected. This is why gingivitis is reversible: no structural damage has occurred.
How Common Is Gingivitis?
Remarkably common. A study in the Journal of Dental Research (2015) estimated that 50-90% of adults worldwide have gingivitis to some degree. In many cases, it's so mild that people live with it for years without realizing it.
What Is Periodontitis?
Periodontitis occurs when gingivitis progresses to involve the deeper structures that support teeth: the periodontal ligament, cementum, and alveolar bone. Unlike gingivitis, the damage from periodontitis is irreversible.
Symptoms of Periodontitis
- All gingivitis symptoms plus:
- Deep periodontal pockets — Spaces between tooth and gum exceed 3mm
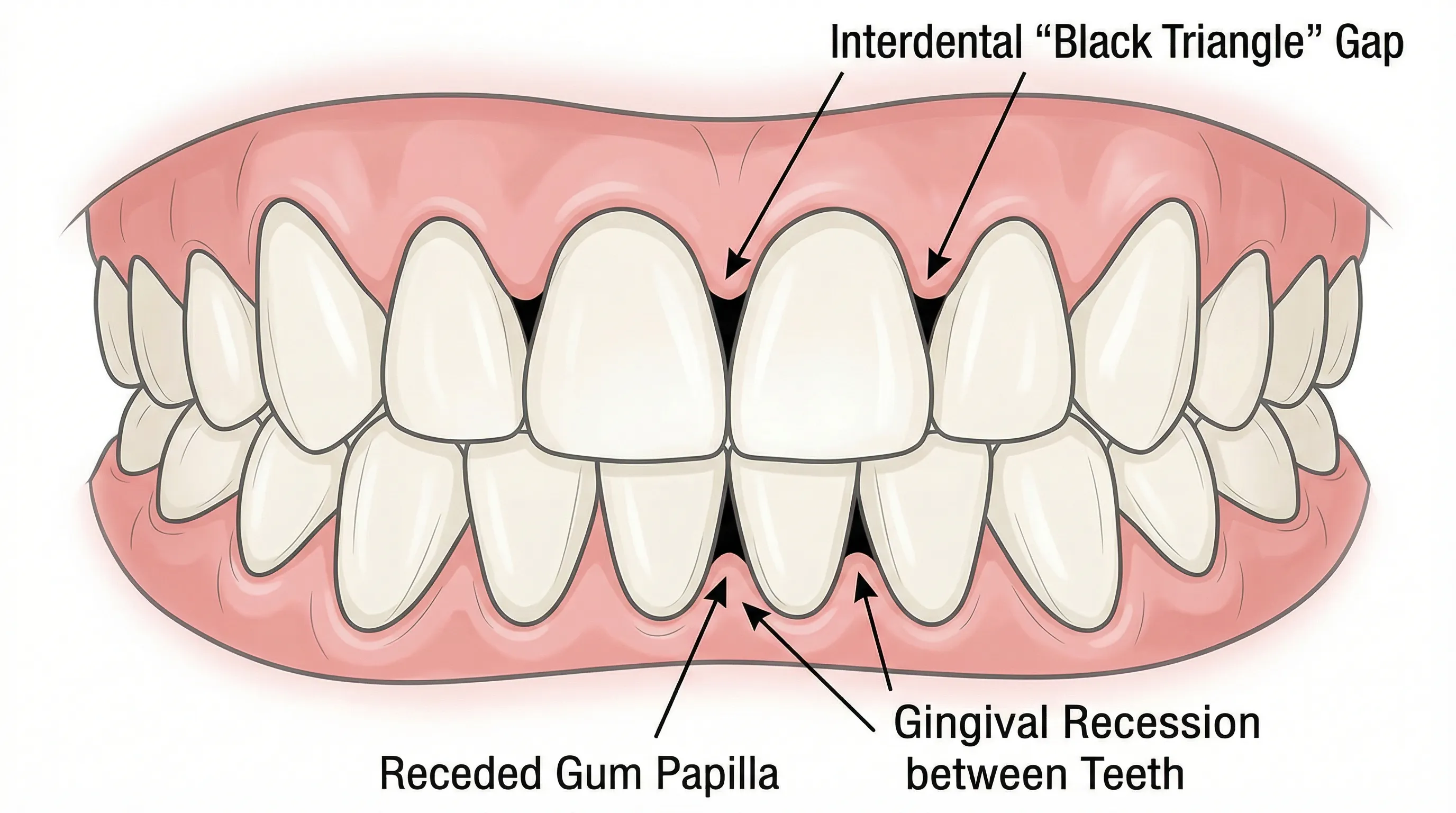
- Gum recession — Gums pull away from teeth, exposing root surfaces
- Bone loss visible on dental X-rays
- Tooth mobility — Teeth may feel loose as bone support erodes
- Pus between teeth and gums (in acute phases)
- Shifting teeth — Gaps may appear as teeth move position
- Changes in bite alignment
- Tooth loss — The end stage if untreated
What's Happening at the Tissue Level
When gingivitis is left untreated, certain aggressive bacterial species — particularly Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola (the "Red Complex") — colonize the deepening pockets below the gumline.
The progression:
- Pocket deepening — Inflammation destroys the junctional epithelium seal, creating deeper spaces between tooth and gum
- Connective tissue destruction — Bacterial enzymes (collagenases, matrix metalloproteinases) break down the collagen fibers that attach gum tissue to tooth root
- Bone resorption — The inflammatory response triggers osteoclast activation, causing the alveolar bone to dissolve
- Biofilm maturation — The deeper pockets create an anaerobic (oxygen-free) environment that favors the most destructive bacterial species
- Self-perpetuating cycle — More destruction creates deeper pockets, which harbor more bacteria, causing more destruction
This is why periodontitis requires professional intervention — the cycle cannot be broken by home care alone once pockets exceed 4-5mm.
Periodontitis Classification
The 2017 World Workshop on Periodontal Classification revised the staging system:
Stage I (Initial): Pocket depths 4mm, 1-2mm clinical attachment loss, no tooth loss Stage II (Moderate): Pocket depths 5mm, 3-4mm attachment loss, no tooth loss Stage III (Severe): Pocket depths 6mm+, 5mm+ attachment loss, tooth loss possible Stage IV (Advanced): Extensive tooth loss, bite collapse, need for complex rehabilitation
Additionally, periodontitis is graded by progression rate:
- Grade A: Slow progression
- Grade B: Moderate progression
- Grade C: Rapid progression
The Tipping Point: When Gingivitis Becomes Periodontitis
Not all gingivitis progresses to periodontitis. The transition depends on several factors:
Risk Factors That Accelerate Progression
- Smoking — The strongest modifiable risk factor. Smokers are 2-6x more likely to develop periodontitis (Journal of Periodontology, 2018)
- Diabetes — Poorly controlled blood sugar dramatically increases periodontitis risk and severity. The relationship is bidirectional — periodontitis also worsens glycemic control.
- Genetics — Approximately 30% of the population may be genetically susceptible to periodontitis regardless of hygiene habits (Journal of Clinical Periodontology, 2015)
- Stress — Chronic stress impairs immune function and is associated with increased periodontal destruction
- Poor nutrition — Vitamin C and D deficiency weaken gum tissue defenses
- Immune compromise — HIV, immunosuppressive medications, and certain systemic conditions increase risk
The Timeline
In susceptible individuals, gingivitis can progress to early periodontitis within months. In others, it may take years or never progress at all. Regular dental monitoring is the only reliable way to catch the transition early.
Treatment: Gingivitis vs. Periodontitis
Treating Gingivitis
Gingivitis treatment is straightforward and can often be done at home:
- Improved brushing technique — Soft-bristle brush, 45-degree angle, gentle circular motions, 2 minutes twice daily
- Daily flossing — Removes plaque from between teeth where brushing misses
- Professional cleaning — If calculus (tartar) has formed, a dental hygienist needs to remove it
- Antimicrobial rinse — Chlorhexidine mouthwash may be recommended short-term
Timeline: Gingivitis typically resolves within 2-4 weeks of consistent improved hygiene. Your dentist should confirm resolution at a follow-up visit.
Treating Periodontitis
Periodontitis treatment is more involved and always requires professional care:
Non-surgical treatment:
- Scaling and root planing (SRP) — Deep cleaning below the gumline to remove plaque, calculus, and bacterial toxins from root surfaces. This is the gold-standard first-line treatment.
- Local antibiotics — Minocycline or doxycycline microspheres may be placed directly into deep pockets
- Systemic antibiotics — Occasionally prescribed for aggressive or widespread periodontitis
Surgical treatment (for cases not responding to SRP):
- Flap surgery — Gums are lifted to allow direct access for cleaning deep pockets and reshaping bone
- Bone grafting — Replaces bone lost to periodontitis
- Guided tissue regeneration (GTR) — Uses barrier membranes to direct new bone and tissue growth
- Gum grafting — Treats recession by transplanting tissue to cover exposed roots
Maintenance: Periodontitis patients typically need professional cleanings every 3-4 months (rather than the standard 6 months) indefinitely. This is called supportive periodontal therapy (SPT) and is critical for preventing recurrence.
Prevention: Keeping Gingivitis from Becoming Periodontitis
The single most important prevention strategy: don't let gingivitis go untreated.
Practical prevention:
- Brush properly twice daily — Removes 60% of plaque
- Floss daily — Removes the remaining 40% between teeth
- Regular dental visits — Every 6 months for examination and professional cleaning
- Don't smoke — Smoking is the most impactful modifiable risk factor
- Manage blood sugar — If diabetic, tight glycemic control protects gums
- Eat well — Vitamin C, vitamin D, and omega-3 fatty acids support gum health
The Role of Oral Probiotics
Oral probiotics represent a newer approach to supporting gum health alongside traditional hygiene measures. Research suggests they can help at both stages:
For gingivitis: A systematic review in Nutrients (2021) found that probiotic supplementation reduced gingival inflammation markers and improved plaque index scores.
For periodontitis: L. reuteri supplementation as an adjunct to scaling and root planing improved clinical outcomes compared to SRP alone (Journal of Clinical Periodontology, 2020).
Probiotics don't replace any of the treatments above — they complement them by helping establish a healthier oral microbiome that's more resistant to pathogenic colonization.

ProDentim
Oral Probiotic for Gum & Teeth Health
ProDentim's L. reuteri strain has been studied as an adjunct to both gingivitis and periodontitis treatment, with improvements in bleeding and pocket depth outcomes.
We may earn a commission if you make a purchase through our links, at no extra cost to you.
A Note on Self-Diagnosis
You cannot reliably distinguish gingivitis from early periodontitis on your own. The symptoms overlap significantly, and the critical difference — bone loss — is only visible on dental X-rays. Periodontal pocket measurements require a dental probe.
If your gums bleed, see your dentist for a proper evaluation. The difference between "just gingivitis" and "early periodontitis" determines your treatment path and long-term prognosis.